-2")
The Mooreville II
Double-Bladed Advanced Cavernotome
Dr. Mooreville is available to answer by email or a telephone conversation can be scheduled.
uramix@comcast.net
+1 610.394.9850
Key Benefits
Easier and faster creation of an intracorporeal space in scarred genitalia from previous surgery or disease (i.e. – Peyronie’s, Sickle Cell). The cavernotome is great at removing bacterial film from previously infected corpora.
Method of Use
A new double-bladed cavernotome with improved coring ability and ease of use.
- Entry to fibrotic corpora needs to be accessed by scalpel & extended both proximally & distally to allow entry to dilator
- Working element should initially be directed laterally
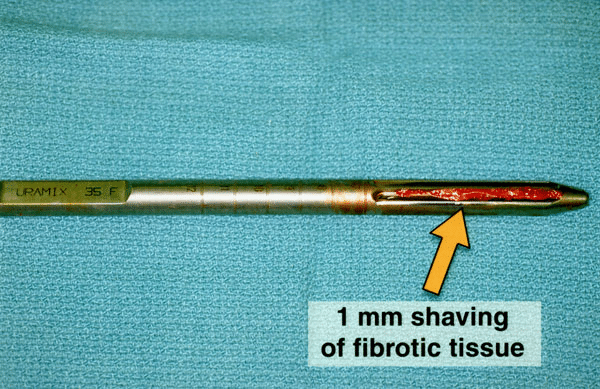
- Cutting of fibrotic tissue can be obtained longitudinally & also in a rotating shaving action
- Dilators are used in succession to the desired size
- Dilators can be used in nonfibrotic corpora for speedier dilation
Method of Use
A new double-bladed cavernotome with improved coring ability and ease of use.
- Entry to fibrotic corpora needs to be accessed by scalpel & extended both proximally & distally to allow entry to dilator
- Working element should initially be directed laterally
- Cutting of fibrotic tissue can be obtained longitudinally & also in a rotating shaving action
- Dilators are used in succession to the desired size
- Dilators can be used in nonfibrotic corpora for speedier dilation
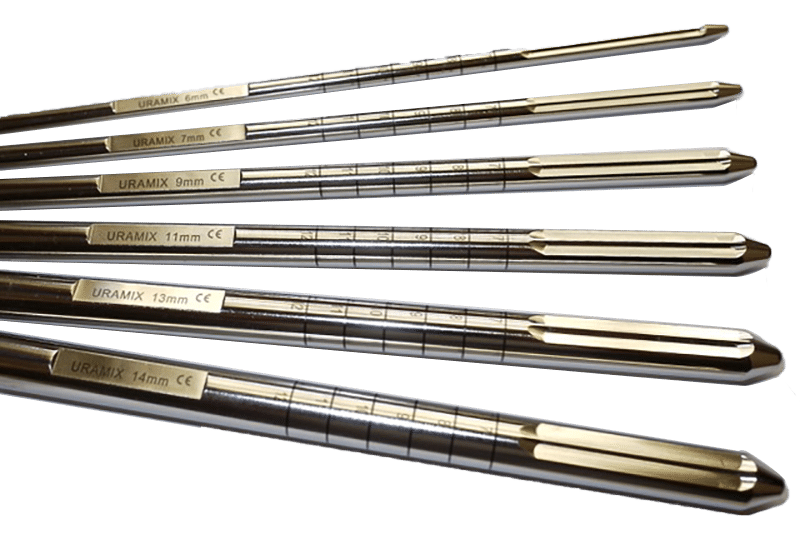
Features Overview
Top grade surgical steel, does not need resharpening
Both the instrument and the handle are autoclavable
6 cavernotomes with diameters between 6, 7, 8, 9, 10, and 11 mm
3 cavernotomes with diameters between 12, 13, and 14mm
Cavernotomes can also be used as a measuring tool
2 parallel blades of 5 cm
23.5 cm

Additional handle for increased torque in difficult dilations, flat surface on the same plane as the blade for ease of orientation
Easily mountable and removable for use and cleaning as well as fixed handle instruments
Rounded protective tip
Height of blade does not exceed circumference of the dilator
Two blades advanced to within 0.5 cm of the tip
EVA cases, combining the protection of a hard case with the versatility and portability of a soft case
Pricing
$2,899 for full set (6)
$2,699 for any five
$2,399 for any four
$1,999 for any three
$1,999 for X-Large set (3),
$4,299 for the full set (6) and X-tra large set (3)
Fixed handle SKU # FH9907 | Removable handle SKU # RH9007
Case study
The cavernotomes were used in nineteen patients with corporeal fibrosis. The etiology of the fibrosis was removal of previously infected prosthesis (15), extensive fibrosis from recurrent priapism secondary to sickle cell disease (2), pharmacologic injection program and subsequent Winter shunts (2). One of the patients whose prosthesis was removed for infection also had a tip erosion on the contralateral side necessitating the creation of a subcapsular space for the insertion of a new cylinder.
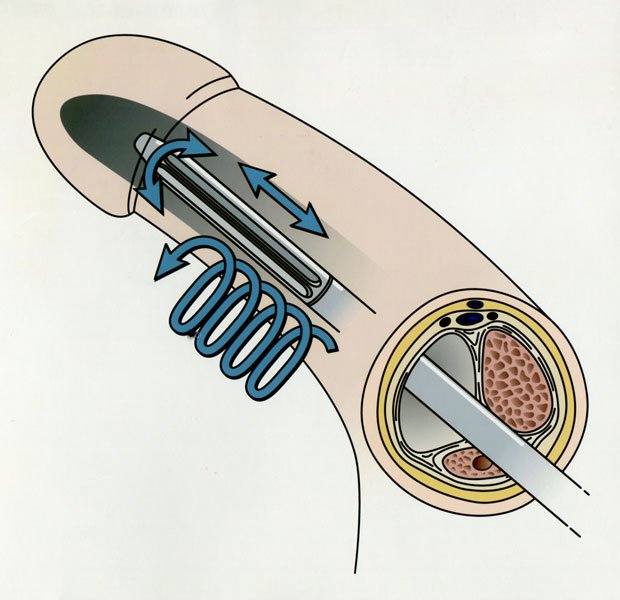
Surgical Technique
After a small corporotomy is created, the cavernotomes are introduced and moved in an oscillating motion resulting in forward advancement. If more resection is needed, rotation of the cavernotomes will create a “shaving” action which removes 1 mm strips of fibrotic tissue.
- Cutting can be done both in a longitudinal, up and down, movement, or in a “drilling” rotational movement.
- The largest size (13 mm) corresponds to standard cylinder diameter. Dilation to 10 mm is necessary for insertion of the Furlow tool or the Mentor NB cylinder base. Dilation to 11 mm is necessary for the insertion of the AMS CXM base.
- Internal cutting of the fibrosis obviates extensive corporotomies and results in quicker procedures.
- The cavernotome’s design and oscillating advancement promote safe dilation without perforation.
Cavernotome being used to dilate fibrotic corpora
All uses of the cavernotomes resulted in successful implantation of inflatable cylinders or semimalleable rods without urethral injury or corporal perforation.
- Fifteen of the patients received downsized prosthesis (13 Alpha NB, 2 AMS 700 CXM).
- Of the remaining four patients, three patients were implanted with Mentor Alpha 1 standard size cylinders, and 1 patient was implanted with an AMS semimalleable prosthesis.
- Graft material was not required and only two patients required additional distal penile incisions for optimum cylinder tip placement.
- Average operative time was 51 minutes (39-86 minutes range).
As seen in Wilson’s Perils and Pitfalls of Penile Prosthesis Surgery, Tobias S. Kohler, MD, Nikhil Gupta, MD, Steven K. Wilson, MD, 2nd edition, January 2018
references
Bruce B. Garber, Caitlin Lim. “Inflatable Penile Prosthesis Insertion in Men with Severe Intracorporal Fibrosis.” Current Urology (2017) 10:92–96.
Michael Mooreville, Sorin Adrian, John R. Delk, and Steven K. Wilson. “Implantation of Inflatable Penile Prosthesis in Patients with Severe Corporeal Fibrosis: Introduction of a New Penile Cavernotome.” The Journal of Urology 162 (1999).
Steve K. Wilson. “Reimplantation of inflatable penile prosthesis into scarred corporeal bodies”. International Journal of Impotence Research (2003) 15, Suppl 5, S125-S128.
place an order
Fill out the information required and we will be in touch to continue the order process.