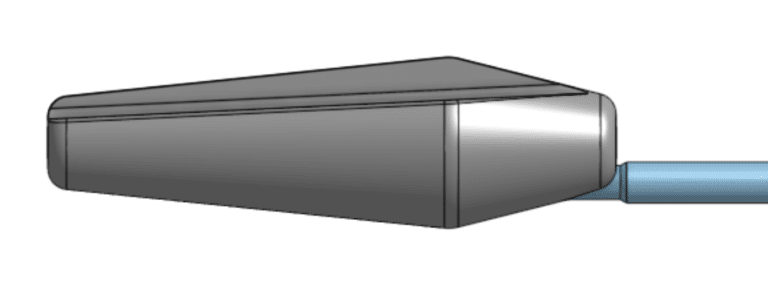
The Mooreville Urethrotome
The Otis Urethrotome simplified
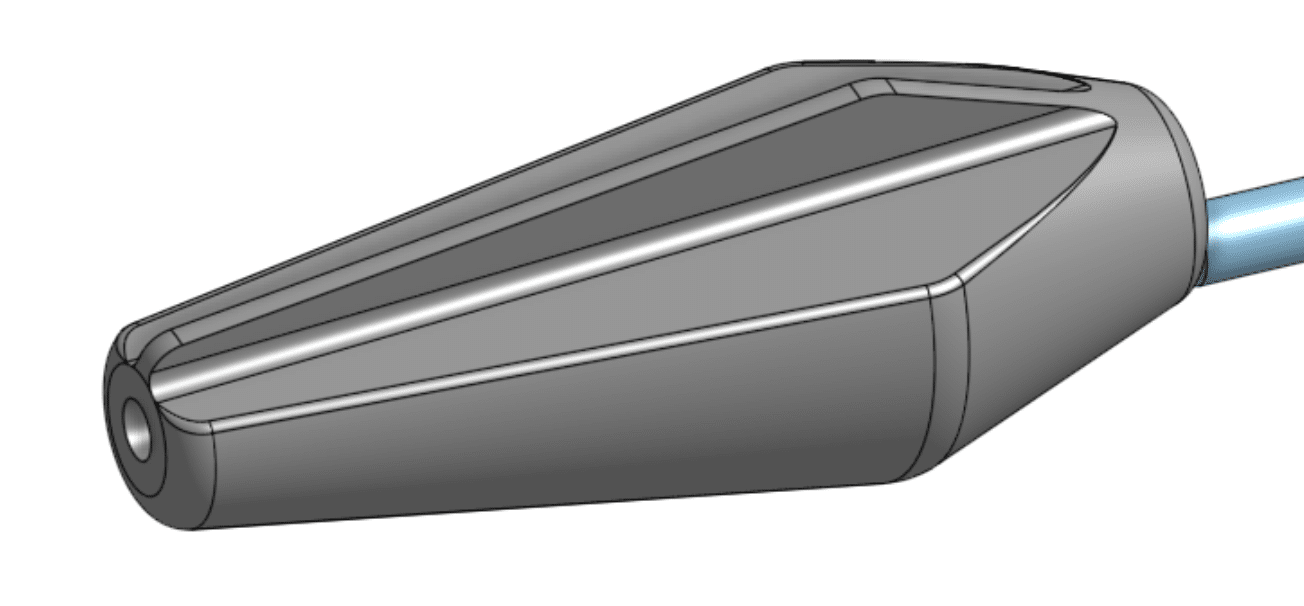
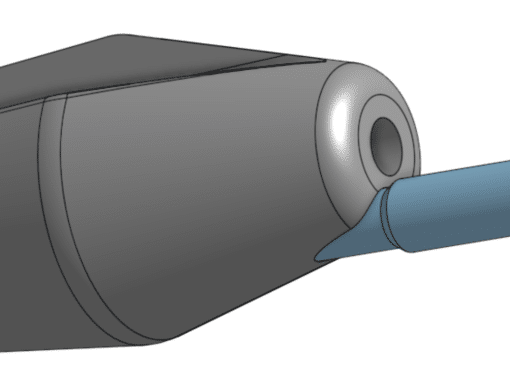
The new urethrotome allows for easy and safe non-visual internal urethrotomy by passage over a guidewire, no moving parts and cutting of only fibrous scar. The flat blade protects normal urethra, which is pushed gently away during passage.
Dr. Mooreville is available to answer by email or a telephone conversation can be scheduled.
sales@uramix.com
+1 610.394.9850
Key Benefits
Easy to use in multiple settings. Improved reimbursement.
Method of Use
Initially, after the instillation of an urethral anesthetic lubricant, a guide wire is passed into the urethra and through the stricture to the bladder. The urethrotome is loaded over the guidewire and slid gently to the stricture, which will be noted by increased resistance to the passage over the guide wire through the tactile feedback characteristic of the stem. Normal tissue is gently pushed out of the way. Markings on the stem will help localize the depth of the stricture from the meatus.
Advancing the urethrotome through the stricture will gently stretch fibrous bands, which will then be exposed to the sharp square edges of the urethrotome and divided as the urethrotome is advanced through the stricture. The 8-12 F and 10-20 F urethrotomes are enough for most strictures. They can also be used for bladder neck stenosis status post radical prostatectomy.
Features Overview
Top grade surgical steel, does not need resharpening
Both the instrument and the handle are autoclavable
2 different sizes, 8 – 14 F and 10 – 20 F. An extra large 12-26F urethrotome is available for meatotomies to allow a 26F resectoscope.
“CM” markings on the stem of the instrument to help assess the depth of the stricture. “Double” markings at 5, 10 and 15 cm
Flexible stem with tactile feedback characteristics.
Central hole for passage over a guidewire
Height of blade does not exceed circumference of the cone
Pricing
$1,599 for full set (2) 8-14F and 10-20F
SKU #4401
Extra large (12-26F): $799
SKU # 4402
Shipping: $50
Patent # 10,500,379
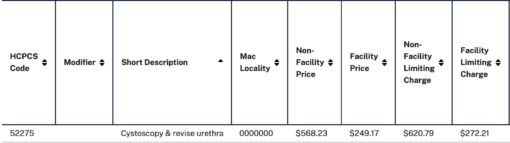
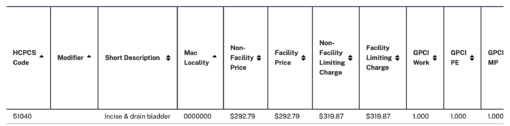
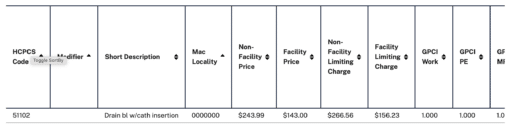
52275 – Internal Urethrotomy Code (2022)
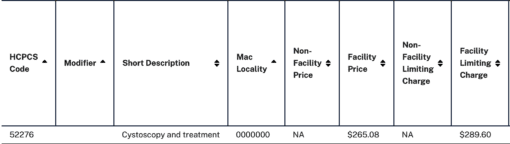
52276 – DVIU Code (2022)
Uramix does not endorse any particular code for billing purposes. These codes are only provided for information purposes.
1,2,3 cms.gov
references
Suprapubic tract dilation using the Otis urethrotome. Thrasher JB, Kreder KJ. Urology. 1993 Mar; 41(3):247-8.
https://www.ncbi.nlm.nih.gov/pubmed/8442308
Percutaneous nephrostomy tract incision using a modified Otis urethrotome. Ireton RC. Urology Clinics of North Am. 1990 Feb; 17(1):195-8
https://www.ncbi.nlm.nih.gov/pubmed/2305529
place an order
Fill out the information required and we will be in touch to continue the order process.